January 4 – A study published in Circulation titled “Circulating Spike Protein Detected in Post-COVID-19 mRNA Vaccine Myocarditis” finds while “antibody profiling and T-cell responses in the individuals who developed postvaccine myocarditis were essentially indistinguishable from those of vaccinated control subjects… markedly elevated levels of full-length spike protein, unbound by antibodies, were detected in the plasma of individuals with postvaccine myocarditis.” Doctors believe the free spike antigens (toxins) detected in the blood of those who developed myocarditis after being vaccinated could offer insight into the underlying causes of the condition, though they still don’t understand why inflammation occurs in some people and not others.
January 24 – Frontiers in Psychology publishes an article titled, “Post COVID-19, still wear a face mask? Self-perceived facial attractiveness reduces mask-wearing intention.” According to South Korea’s Department of Psychology and Center for Happiness Studies, the results of several studies “consistently demonstrated that self-perceived unattractive individuals were more willing to wear a mask, as they believed it would benefit their attractiveness.” Also see this UK Daily Mail breakdown for more details.
January 26 – Doctors from the US and UK publish a preprint study at the medRxiv website showing Merck’s COVID treatment Lagevrio is causing mutations that could lead to deadlier COVID strains in the future. According to Bloomberg, Lagevrio works by creating mutations in the Covid genome that prevent the virus from replicating in the body, reducing the chances it will cause severe illness. Some scientists had warned before it was authorized in late 2021 that by virtue of how it works, the drug could give rise to mutations that could turn out to be problematic. The preprint paper has reawakened those worries about the Merck drug. ‘There’s always been this underlying concern that it could contribute to a problem generating new variants,’ said Jonathan Li, a virologist at Harvard Medical School and Brigham and Women’s Hospital in Boston. ‘This has largely been hypothetical, but this preprint validates a lot of those concerns.’” Though Merck disputes these claims, the study found “Lagevrio-induced mutations in small patient clusters, indicating the new versions were spreading among them. While the biggest group they found with similar mutations was 21 people, that may not fully represent the true scope of the problem as viral samples of many patients aren’t analyzed, according to Ryan Hisner, an independent researcher from Indiana who helped write the paper. The researchers looked at some 13 million viral genomes in databases around the world. The drug-linked mutations were proportionally more common in countries and groups where Lagevrio was likely to be used, especially the US and Australia, where it was introduced early. The signature mutations are less frequent in Canada, France, and other countries where the drug isn’t used.”
January 30 – Cochrane publishes a review on masks titled, “Physical interventions to interrupt or reduce the spread of respiratory viruses.” The 326-page meta-analysis includes the results of 78 randomized controlled trials (RCTs) from around the world. The study found “the pooled results of RCTs did not show a clear reduction in respiratory viral infection with the use of medical/surgical masks. There were no clear differences between the use of medical/surgical masks compared with N95/P2 respirators in healthcare workers when used in routine care to reduce respiratory viral infection.” In other words, masks do diddly squat when it comes to preventing respiratory illnesses. Here’s a link to the much shorter abstract. Update (3/10/23): Editor-in-Chief of the Cochrane Library, Karla Soares-Weiser, issues a statement regarding their mask review, claiming the results have been misinterpreted. The statement reads in part, “Many commentators have claimed that a recently-updated Cochrane Review shows that ‘masks don’t work’, which is an inaccurate and misleading interpretation. It would be accurate to say that the review examined whether interventions to promote mask wearing help to slow the spread of respiratory viruses, and that the results were inconclusive. Given the limitations in the primary evidence, the review is not able to address the question of whether mask-wearing itself reduces people’s risk of contracting or spreading respiratory viruses… The original Plain Language Summary for this review stated that ‘We are uncertain whether wearing masks or N95/P2 respirators helps to slow the spread of respiratory viruses based on the studies we assessed.’ This wording was open to misinterpretation, for which we apologize. While scientific evidence is never immune to misinterpretation, we take responsibility for not making the wording clearer from the outset. We are engaging with the review authors with the aim of updating the Plain Language Summary and abstract to make clear that the review looked at whether interventions to promote mask wearing help to slow the spread of respiratory viruses.” I have to believe Soares-Weiser was pressured by a representative of the death cult to issue this statement. Masks have been a powerful tool used to psychologically manipulate and divide the masses, and so they’re never going to give that up if possible. Moreover, the initiation ritual isn’t over yet. But whether or not Cochrane’s editor-in-chief can tell the truth about masks is meaningless, because I sure as hell still can! Masks do jack shit when it comes to preventing and spreading respiratory illnesses, and all the proof you will ever need can be found here.
February 16 – The Lancet publishes a study titled, “Past SARS-CoV-2 infection protection against re-infection: a systematic review and meta-analysis” – which, surprisingly, was funded by the Bill and Melinda Gates Foundation. The “findings” section reads, “We identified a total of 65 studies from 19 different countries. Our meta-analyses showed that protection from past infection and any symptomatic disease was high for ancestral, alpha, beta, and delta variants, but was substantially lower for the omicron BA.1 variant. Pooled effectiveness against re-infection by the omicron BA.1 variant was 45·3% (95% uncertainty interval [UI] 17·3–76·1) and 44·0% (26·5–65·0) against omicron BA.1 symptomatic disease. Mean pooled effectiveness was greater than 78% against severe disease (hospitalisation and death) for all variants, including omicron BA.1. Protection from re-infection from ancestral, alpha, and delta variants declined over time but remained at 78·6% (49·8–93·6) at 40 weeks. Protection against re-infection by the omicron BA.1 variant declined more rapidly and was estimated at 36·1% (24·4–51·3) at 40 weeks. On the other hand, protection against severe disease remained high for all variants, with 90·2% (69·7–97·5) for ancestral, alpha, and delta variants, and 88·9% (84·7–90·9) for omicron BA.1 at 40 weeks.” Unsurprisingly, these positive findings are immediately followed up with, “The immunity conferred by past infection should be weighed alongside protection from vaccination when assessing future disease burden from COVID-19, providing guidance on when individuals should be vaccinated, and designing policies that mandate vaccination for workers or restrict access, on the basis of immune status, to settings where the risk of transmission is high, such as travel and high-occupancy indoor settings.” The word “alongside” is defined as “together and in cooperation with” and “at the same time as or in coexistence with.” In other words, even if you’ve already had COVID and have adequate protection against re-infection, go ahead and roll up that sleeve anyway.
March 13 – Current Biology publishes a nonsensical study titled, “A meta-analysis of the associations between insufficient sleep duration and antibody response to vaccination.” Some of the highlights of the study – or lowlights, depending on how you look at it – are 1) “Insufficient sleep (<6 hours/night) around vaccination reduces the antibody response,” 2) “The reduction is similar to the waning of COVID-19 vaccine antibodies over 2 months,” 3) “The association seems robust in men, but more data are needed in women,” and 4) “Optimizing sleep duration around the time of vaccination may boost antibody response.” Mind-blowing stuff, right? The authors go on to say, “These results provide evidence that insufficient sleep duration substantially decreases the response to anti-viral vaccination and suggests that achieving adequate amounts of sleep during the days surrounding vaccination may enhance and prolong the humoral response. Large-scale well-controlled studies are urgently needed to define (1) the window of time around inoculation when optimizing sleep duration is most beneficial, (2) the causes of the sex disparity in the impact of sleep on the response, and (3) the amount of sleep needed to protect the response.” So it’s not that the shots are garbage and don’t protect people from COVID, people just aren’t getting enough sleep… got it. Also see this and this.
March 20 – A study out of Japan is published at the NIH’s PubMed website titled, “A case of fatal multi-organ inflammation following COVID-19 vaccination.” The “case report” section reads in part, “A 14-year-old Japanese girl received a third dose of the BNT1262b2 mRNA COVID-19 vaccine/Pfizer (Comirnaty®) on 10th August 2022. Despite her history of orthostatic dysregulation, she was healthy by nature and was active in her middle school athletic team. The day after vaccination, she developed a fever of 37.9 °C, which resolved by the same evening. Her sister, who had slept with her that night, reported that she woke up briefly because she was having difficulty in breathing, talked with her sister, and went to bed soon after. The following morning, her mother noticed that she was not breathing and had a pale appearance, and she immediately called an ambulance. The patient was in cardiopulmonary arrest when the ambulance crew arrived at their house and attempts to administer advanced life support were unsuccessful. She died 45 h after the third vaccination.” So I’ll ask for the thousandth time: Why are young healthy children being injected with this garbage when COVID is not a danger to them?
May 17 – A study is published at the Multidisciplinary Digital Publishing Institute (MDPI) website titled, “IgG4 Antibodies Induced by Repeated Vaccination May Generate Immune Tolerance to the SARS-CoV-2 Spike Protein.” The abstract reads in part, “To date, 72.3% of the total population has been injected at least once with a COVID-19 vaccine. As the immunity provided by these vaccines rapidly wanes, their ability to prevent hospitalization and severe disease in individuals with comorbidities has recently been questioned, and increasing evidence has shown that, as with many other vaccines, they do not produce sterilizing immunity, allowing people to suffer frequent re-infections. Additionally, recent investigations have found abnormally high levels of IgG4 in people who were administered two or more injections of the mRNA vaccines… It has been suggested that an increase in IgG4 levels could have a protecting role by preventing immune over-activation, similar to that occurring during successful allergen-specific immunotherapy by inhibiting IgE-induced effects. However, emerging evidence suggests that the reported increase in IgG4 levels detected after repeated vaccination with the mRNA vaccines may not be a protective mechanism; rather, it constitutes an immune tolerance mechanism to the spike protein that could promote unopposed SARS-CoV2 infection and replication by suppressing natural antiviral responses. Increased IgG4 synthesis due to repeated mRNA vaccination with high antigen concentrations may also cause autoimmune diseases, and promote cancer growth and autoimmune myocarditis in susceptible individuals.”
The body of the study goes on to say, “Contemporary investigations have contrasted the seriousness of symptoms in COVID-19 individuals infected with the SARS-CoV-2 Alpha, Delta, and Omicron variants, as well as the effectiveness of mRNA immunizations versus each variant among individuals admitted to hospitals in the United States from March 2021 to January 2022… It is worth noting that there are conflicting pieces of information about the level of protection offered by these vaccines. Although the Center for Disease Control (CDC) in the United States has stated that throughout the pandemic, mortality rates have been higher in the unvaccinated than in the vaccinated, the data in the United Kingdom contradict the CDC’s findings. Specifically, the Office for National Statistics (ONS) in the United Kingdom has reported that from April to mid-November 2021, deaths in unvaccinated people were higher in comparison with vaccinated people who had received a second vaccine dose. However, from the end of November 2021 to December 2022, this situation reverted: deaths were higher in vaccinated people who received a third vaccine dose compared with the unvaccinated. Moreover, a recent work investigated a probable relationship between COVID-19 vaccination uptake in Europe in 2021 and monthly excess all-cause mortality in 2022; that is, mortality was higher than before the pandemic. All-cause mortality during the first 9 months of 2022 increased more in countries with higher 2021 vaccination uptake, according to analyses of 31 countries estimated by population size; a one percentage point increase in 2021 vaccination uptake was associated with a monthly mortality increase in 2022 of 0.105%. The relationship remained strong after adjusting for alternative factors.
“Although they can induce significant neutralizing anti-spike IgG and IgA responses, all three anti-COVID-19 vaccines: Pfizer, Moderna, and Astra Zeneca ChAdOx1, (Cambridge, UK) appeared to be only transiently protective against SARS-CoV-2 infection and transmission. The high rate of breakthrough infections brought on by the Omicron variant suggests that the sterilizing protection offered by the existing immunization schedules is minimal… Lethal COVID-19 cases have been linked to higher levels of IgG4 antibodies, and it has also been documented that mRNA vaccines trigger their synthesis. It is, therefore, important to analyze this issue in depth. In this paper, we provide the scientific rationale suggesting that repeated vaccination with mRNA vaccines could generate an immune tolerance mechanism, thereby favoring unopposed SARS-CoV-2 replication. The long-term consequence of this tolerance could be the establishment of a permissive state of the host leading to chronic infection and other unintended consequences induced by mRNA vaccination in susceptible individuals.
“An extensive review of the literature showed that mRNA vaccines are not the only ones that induce IgG4 antibody production. The HIV, Malaria, and Pertussis vaccines also elicited such a response. Overall, there are three critical factors determining the class switch to IgG4 antibodies: excessive antigen concentration, repeated vaccination, and the type of vaccine used. Compared to BNT162b2 [Pfizer], the mRNA-1273 [Moderna] vaccine had a greater capability for inducing a prolonged IgG4 response. The amount and duration of the spike protein produced are presumably affected by the higher mRNA concentrations in the mRNA-1273 vaccine (100 µg) compared to the BNT162b2 vaccine (30 µg)… Immune tolerance may develop as a result of prolonged antigen exposure. T cells are an essential part of the immune system that detects and removes infections and other foreign objects. Yet, these T cells may become desensitized and lose their capacity to react to repeated exposures when they are exposed to large concentrations of antigens, such as during repeated vaccination. Immune tolerance is a condition that can also result in the persistence of infections or the emergence of autoimmune diseases… T cells can undergo a process known as ‘terminal differentiation’ when vaccines are given in high concentrations, at which point they become highly specialized, losing the capacity to divide and proliferate. The immune system becomes exhausted as a result and is unable to mount a successful defense against subsequent illnesses. This is a problem since it might undermine the protective advantages of vaccinations. To balance the advantages of immunological protection and the potential disadvantages of immune exhaustion, it is crucial to carefully determine the ideal dose of vaccines… Adverse outcomes are more likely to occur in groups receiving greater doses.
“We propose a hypothetical immune tolerance mechanism induced by mRNA vaccines, which could have at least six negative unintended consequences: (1) By ignoring the spike protein synthesized as a consequence of vaccination, the host immune system may become vulnerable to re-infection with the new Omicron subvariants, allowing for free replication of the virus once a re-infection takes place. In this situation, we suggest that even these less pathogenic Omicron subvariants could cause significant harm and even death in individuals with comorbidities and immuno-compromised conditions. (2) mRNA and inactivated vaccines temporally impair interferon signaling, possibly causing immune suppression and leaving the individual in a vulnerable situation against any other pathogen. In addition, this immune suppression could allow the re-activation of latent viral, bacterial, or fungal infections and might also allow the uncontrolled growth of cancer cells. (3) A tolerant immune system might allow SARS-CoV-2 persistence in the host and promote the establishment of a chronic infection, similar to that generated by the hepatitis B virus, the human immune deficiency virus, and the hepatitis C virus. (4) The combined immune suppression (produced by SARS-CoV-2 infection and further enhanced by vaccination) could explain a plethora of autoimmune conditions, such as cancers, re-infections, and deaths temporally associated with both. It is conceivable that the excess deaths reported in several highly COVID-19-vaccinated countries may be explained, in part, by this combined immunosuppressive effect. (5) Repeated vaccination could also lead to auto-immunity… According to the self-organized criticality theory, when the immune system of the host is continually overstimulated by antigen exposure at concentrations higher than the immune system’s self-organized criticality can tolerate, systemic autoimmunity inevitably occurs. It has been proposed that the amount and duration of the spike protein produced are presumably affected by the higher mRNA concentrations in the mRNA-1273 vaccine (100 µg) compared to the BNT162b2 vaccine (30 µg). Thus, it is probable that the spike protein produced in response to mRNA vaccination is too high and lasts too long in the body. That could overwhelm the capacity of the immune system, leading to autoimmunity… (6) Increased IgG4 levels induced by repeated vaccination could lead to autoimmune myocarditis; it has been suggested that IgG4 antibodies can also cause an autoimmune reaction by impeding the immune system’s ability to be suppressed by regulatory T cells. Patients using immune checkpoint inhibitors alone or in combination have been linked to occurrences of acute myocarditis, sometimes with lethal consequences. As anti-PD-1 antibodies are class IgG4, and these antibodies are also induced by repeated vaccination, it is plausible to suggest that excessive vaccination could be associated with the occurrence of an increased number of myocarditis cases and sudden cardiac deaths.”
According to a separate study published in 2018, IgG-4 related disease “describes a group of fibroinflammatory diseases that affect a variety of tissues resulting in tumor-like effect and/or organ dysfunction.” These illnesses are treated using glucocorticoids – which I have written about or mentioned at various points throughout this timeline – including budesonide (see October 9th, 2021), dexamethasone (June 16th and September 2nd, 2020), hydrocortisone (also September 2nd, 2020), and prednisone (September 1st, 2021). These drugs were being used successfully (also see this) to treat COVID patients as talented doctors in the US and around the world used their knowledge and training to discover ways to battle back against the lab-created bioweapon. Unfortunately, because of archcriminals like Dr. Fauci and Bill Gates, these treatments – along with many others – were suppressed, and those who dared to go against the decrees of Big Pharma and the soulless monsters who front for them ended up jeopardizing everything they ever worked for. Never forget that.
May 22 – Alex Berenson reports on a study published earlier this month out of Sweden that found “Women 45 and over had a high risk of severe vaginal bleeding after receiving mRNA Covid shots” with “a third mRNA dose [raising] the risk of severe, medically diagnosed bleeding episodes by 25-45 percent. Some women required inpatient hospital care.” The study, with a sample size of nearly three million women, included 2,580,007 (87.6%) who took at least one COVID jab and another 1,652,472 (64% of the 87.6%) who took three doses. According to Berenson, “Because of its size and reliance on formal medical diagnoses rather than self-reporting of vaginal bleeding, the study offers the strongest evidence yet that the connection between Covid shots and bleeding is real. Bizarrely, though, the researchers downplayed their own findings when they discussed the paper, which was published in the British Medical Journal. Meanwhile, the Journal of the American Medical Association relegated the study to a three-paragraph summary in its ‘Medical News in Brief’ section – and inaccurately reported that it had not found the jabs caused menstrual changes in women under 45. It did.” Berenson does a great job analyzing study results and discovering how researchers will often distort their own findings to be in accordance with the COVID narrative. This article is no different and is well worth your time.
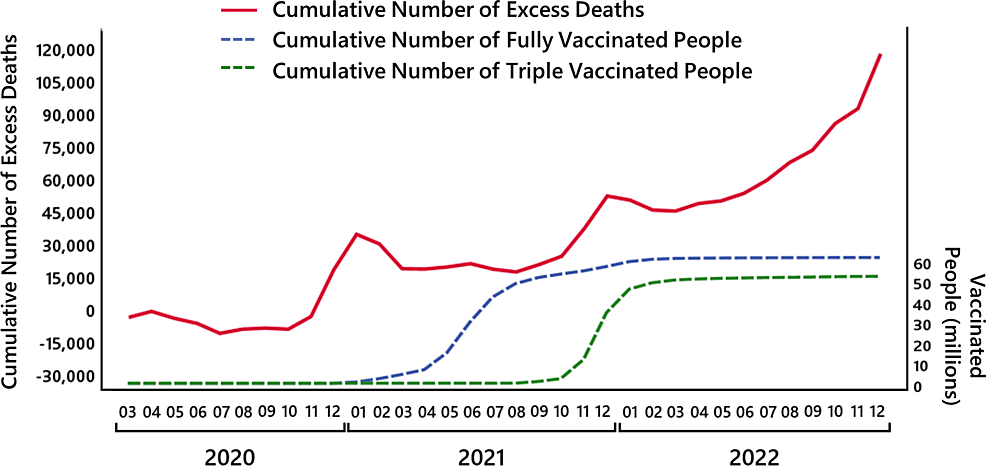
May 23 – A peer-reviewed paper is published in Cureus titled, “Estimation of Excess Mortality in Germany During 2020-2022.” The results show “the observed number of deaths in 2020 was close to the expected number with respect to the empirical standard deviation; approximately 4,000 excess deaths occurred. By contrast, in 2021, the observed number of deaths was two empirical standard deviations above the expected number and even more than four times the empirical standard deviation in 2022. In total, the number of excess deaths in the year 2021 is about 34,000 and in 2022 about 66,000 deaths, yielding a cumulated 100,000 excess deaths in both years. The high excess mortality in 2021 and 2022 was mainly due to an increase in deaths in the age groups between 15 and 79 years and started to accumulate only from April 2021 onward. A similar mortality pattern was observed for stillbirths with an increase of about 9.4% in the second quarter and 19.4% in the fourth quarter of the year 2021 compared to previous years.” In the discussion section of the study, the authors write, “In April 2021, an extensive COVID-19 vaccination campaign started in Germany. Regarding the relationship between excess mortality and vaccinations, if the vaccinations successfully prevent people from dying from COVID-19, a straightforward prediction is that excess mortality should decrease with an increased number of vaccinated persons… As is visible in Figure 8 [shown below], the obvious hypothesis of a decrease in excess mortality with an increasing number of vaccinated persons is not correct. During periods when many persons were vaccinated, excess mortality seems to have increased more strongly compared to the same periods in the previous pandemic year. During the first and second vaccination periods in spring and summer 2021, an increase in cumulative excess mortality is observed, while the year before a decrease was observed. During the period of the third vaccination, parallel to the increase in vaccinations, an increase in cumulative excess mortality can be observed that starts earlier than in the year before. And in 2022, when large parts of the population have been vaccinated, the cumulative number of excess deaths showed a further increase, which even exceeds the previous pandemic year without vaccinations. There seem to be negative long-term effects either of the SARS-CoV-2 infections, COVID-19 measures, the COVID-19 vaccination, or most probably a combination of these.” Most probably a combination of these? Really, guys?
May 27 – Back in March of 2022 a supposed science follower named Dr. Kyle Sheldrick filed a complaint against Dr. Paul Marik – probably due to his approach to COVID and his outspoken support for the use of ivermectin to treat it – accusing him of using fraudulent data in a 2017 study titled “Hydrocortisone, Vitamin C, and Thiamine for the Treatment of Severe Sepsis and Septic Shock: A Retrospective Before-After Study.” Marik’s study was published in the CHEST journal and at PubMed. After a thorough yearlong review, Marik received a letter this past April stating CHEST found his data to contain no methodological errors. A bitter Sheldrick reluctantly published an apology on his blog today saying in part, “On March 22, 2022 I posted a blog post called ‘This Scattrd Corn’. This post was a copy of a complaint I filed with the journal CHEST identifying features of a study led by Paul Marik… Those complaints have since been formally rejected by the journal CHEST, which I consider to be the definitive conclusion to the matter. I realise this letter was used to imply that Dr. Marik personally acted deceptively, and falsely reported study data, which was not my intention, and this caused him significant hurt and distress. I regret this hurt to Dr. Marik. I will inform those who have reported on this complaint that it has been rejected by the journal. Dr. Marik has also indicated to me that some subsequent controlled studies have found some positive outcomes for vitamin C in Sepsis, and I accept this.” Why do I think Sheldrick is bitter? The last line of his apology reads, “This statement is not an endorsement of the use of Vitamin C in sepsis.” LMAO. He doesn’t accept jack shit! Marik has testified at various COVID roundtables and seems to be a genuinely kind person who practices medicine for all the right reasons (unlike The Twerp).
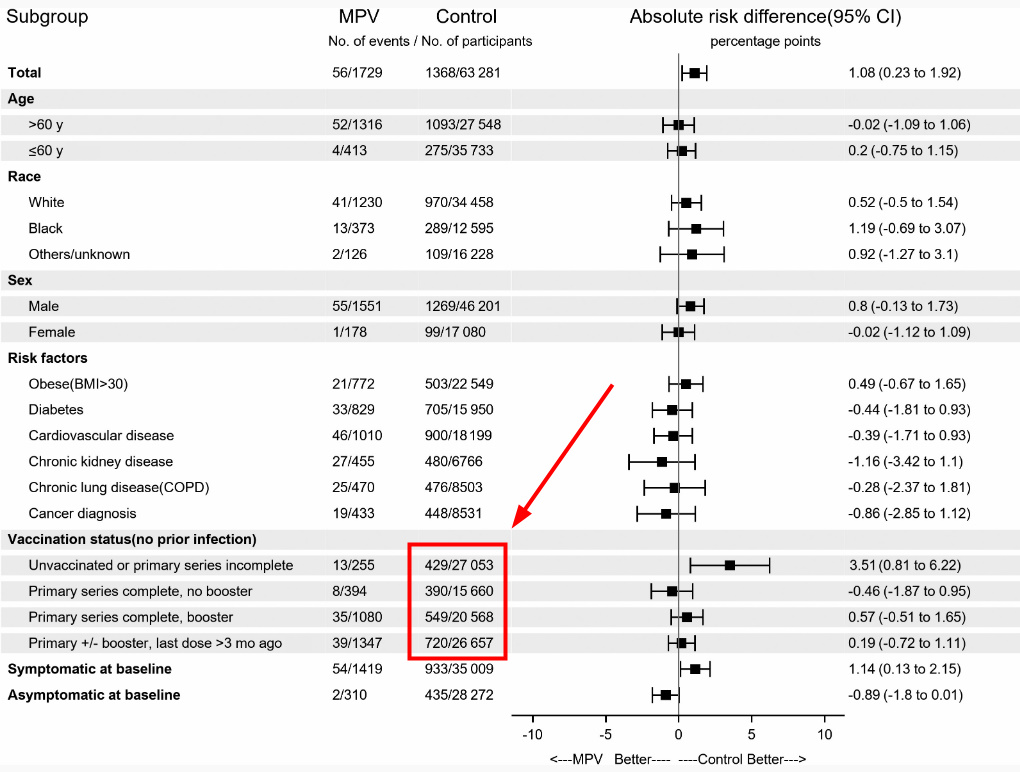
June 1 – A study is published in The Journal of Infectious Diseases titled, “Molnupiravir Use and 30-Day Hospitalizations or Death in a Previously Uninfected Nonhospitalized High-risk Population With COVID-19.” The study looked at how molnupiravir (MPV) – which is made by Merck – worked on 1,459 veterans who received the drug versus over 63,000 veterans who did not. Unsurprisingly, “MPV was not associated with a reduction in hospitalization or death within 30 days of COVID-19 diagnosis.” However, when you dig into the numbers a little bit, you find the people who completed the “primary series” of the COVID vaccine (with or without a booster) generally fared much worse than those in the “unvaccinated or primary series incomplete” category. In fact, the number of COVID hospitalizations and deaths among the “vaccinated” in the control group was nearly double that of the unvaccinated. Data from the study shows the “unvaccinated or primary series incomplete” group were hospitalized or died at a rate of 16 per 1,000 versus 25 per 1,000 for those who took the primary series but no booster, and 27 per 1,000 who completed the primary series and took at least one booster. So while the authors concluded “MPV was not associated with a reduction in hospitalization or death within 30 days of COVID-19 diagnosis,” what we actually have is another study showing us the chance of being hospitalized from or killed by COVID increases with every additional “vaccine” dose taken. Hat tip to Igor Chudov.
June 2 – A study out of South Korea is published titled, “COVID-19 vaccination-related myocarditis: a Korean nationwide study.” The study found the nationwide rate for vaccine-related myocarditis (VRM) to be 1.08 cases per 100,000 people, though the adjudication committee who determined which cases of myocarditis were classified as VRM did so using the “case definition and classification of the Brighton Collaboration (BC).” BC is partnered with CEPI (the Coalition for Epidemic Preparedness Innovations), and CEPI “was founded in Davos by the governments of Norway and India, the Bill & Melinda Gates Foundation, Wellcome, and the World Economic Forum.” So basically all of the biggest funders and promoters of (mostly needless) vaccines created a system to (supposedly) determine whether or not the pharmaceutical products they are relentlessly pushing are hurting people… That doesn’t sound like a very trustworthy system to me, but then again, I’m a kook. But back to the study. Using this flawed system, it was determined that out of 1,533 cases of myocarditis reported to the Korea Disease Control and Prevention Agency, only 480 were classified as vaccine-related myocarditis. Cases were much higher in men than women (1.35 vs. 0.82 per 100,000). Males between the ages of 12 and 17 had the highest rate of VRM (5.29 per 100,000), followed by males ages 18 to 29 (2.93 per 100,000). Women above the age of 70 had the lowest rate of VRM at just 0.16 per 100,000. The study also showed fulminant myocarditis or death occurred in 19.8% of those who suffered from VRM, which is a very high rate. But perhaps the most interesting information revealed by the study were the rates of VRM by vaccine type and brand. The Moderna mRNA jab caused the highest rate of VRM by far at 2.30 per 100K, which was followed by the Pfizer/BioNTech mRNA jab at 1.23 per 100K. The two viral vector vaccines showed much lower rates of VRM, with Johnson & Johnson’s jab coming in at 0.20 per 100K and AstraZeneca’s coming in at 0.14 per 100K. I don’t think it’s a coincidence how the two mRNA “vaccines” were pushed the hardest as they were created with NIH funding and pay royalties to the scientists involved. Even though the viral vector “vaccines” caused VRM at rates much lower than their mRNA counterparts, for a while the public was led to believe the J&J and AZ jabs were the riskier options (“safe and effective” vs. “risk of blood clots”). Clearly this was never the case, but unfortunately science has been partnered with big business for far too long.

June 12 – The pesky science-followers at the Cleveland Clinic are at it again, this time publishing a study titled, “Risk of Coronavirus Disease 2019 (COVID-19) among Those Up-to-Date and Not Up-to-Date on COVID-19 Vaccination.” Not only is the title slightly adversarial, but the introduction is too… “In April 2023 the Centers for Disease Control and Prevention (CDC) updated its guidance on Coronavirus Disease 2019 (COVID-19) vaccination to consider all individuals above the age of 6 to be ‘up-to-date’ with COVID-19 vaccination only if they had received at least one dose of a COVID-19 bivalent vaccine. By this definition, those who had not received a single dose of a COVID-19 bivalent vaccine would be considered not ‘up-to-date.’ A recent study was unable to find the bivalent vaccine to be effective while the XBB variants were the dominant circulating strains. Given this lack of effectiveness of the bivalent vaccine against the XBB variants, which are the predominant circulating strains at this time, it is reasonable to question whether individuals ‘up-to-date’ with a vaccine of questionable effectiveness are protected against COVID-19 compared to those not ‘up-to-date.’ The purpose of this study was to evaluate whether individuals who were not ‘up-to-date’ on COVID-19 vaccination had a higher risk of COVID-19 than those ‘up-to-date.’” The fact these doctors are putting the words “up-to-date” in quotes is a not-so-subtle shot at the supposed “experts” at the CDC. And if that isn’t enjoyable enough, the conclusions and summary sections explain quite concisely why people should stop injecting themselves with these ineffective products immediately… “Conclusions: Since the XBB lineages became dominant, adults ‘not up-to-date’ by the CDC definition have a lower risk of COVID-19 than those ‘up-to-date’ on COVID-19 vaccination, bringing into question the value of this risk classification definition. Summary: Among 48,344 working-aged Cleveland Clinic employees, those not ‘up-to-date’ on COVID-19 vaccination had a lower risk of COVID-19 than those ‘up-to-date.’ The current CDC definition provides a meaningless classification of risk of COVID-19 in the adult population.” The discussion section even takes a dig at the CDC’s unwillingness to consider prior infection as providing protection from COVID, with the authors writing, “There are two reasons why not being ‘up-to-date’ on COVID-19 vaccination by the CDC definition was associated with a lower risk of COVID-19. The first is that the bivalent vaccine was somewhat effective against strains that were more similar to the strains on the basis of which the bivalent vaccine was developed, but is not effective against the XBB lineages of the Omicron variant. The second is that the CDC definition does not consider the protective effect of immunity acquired from prior infection. Because the COVID-19 bivalent vaccine provided some protection against the BA.4/BA.5 and BQ lineages, those ‘not-up-to-date’ were more likely than those ‘up-to-date’ to have acquired a BA.4/BA.5 or BQ lineage infection when those lineages were the dominant circulating strains. It is now well-known that SARS-CoV-2 infection provides more robust protection than vaccination. Therefore it is not surprising that not being ‘up-to-date’ according to the CDC definition was associated with a higher risk of prior BA.4/BA.5 or BQ lineage infection, and therefore a lower risk of COVID-19, than being ‘up-to-date,’ while the XBB lineages were dominant.” Mandy Cohen is officially on notice: Do a better job following the science than your dopey predecessor did.
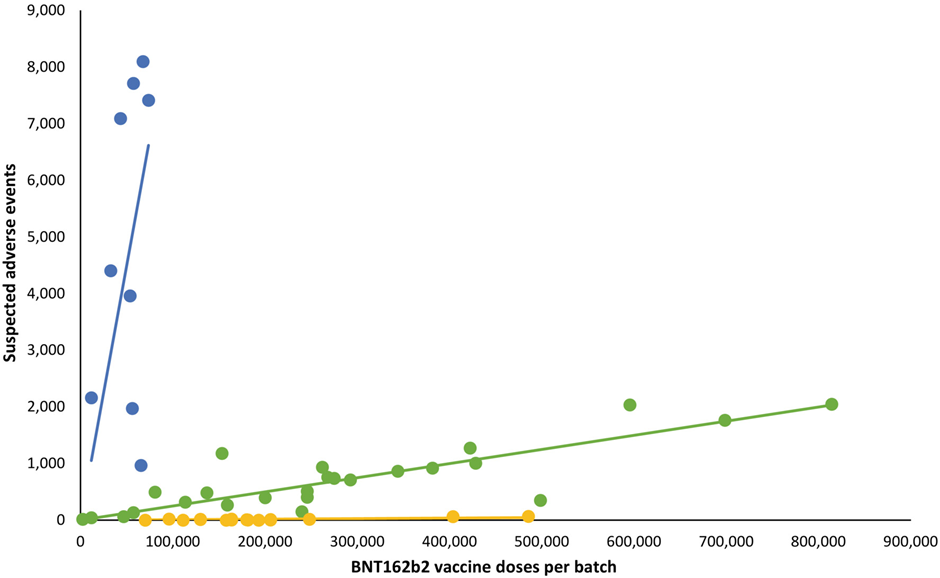
June 28 – The Daily Sceptic publishes an article titled, “Pfizer Vaccine Batches in the EU Were Placebos, Say Scientists.” The article is about a group of German scientists who discovered a large number of the COVID “vaccines” distributed throughout the European Union may have been placebos. Their investigation started after a Danish study published in March of 2023 showed considerable discrepancies in the number of adverse events associated with different batches of the BioNTech COVID vaccine. The batches distributed in Denmark were able to be neatly placed into one of three groups, with 60% of the vaccines used throughout the country coming from the green group (see the graph below). People who received a jab from this group experienced an adverse event at the rate of 1 in 400 – a relatively high number when compared to a seasonal flu vaccine. Out of the 80,000 vaccinations given to Danes from the blue group, up to 8,000 adverse reactions may have occurred, an astonishingly high rate of 1 in 10. According to one of the German scientists, “the blue batches represent less than 5% of the total number of doses included in the Danish study. Nonetheless, they are associated with nearly 50% of the 579 deaths recorded in the sample.” This same scientist also believes these batches were quietly pulled from the market by public health authorities once the injury rate was realized.
Finally, we have the yellow group, which shows almost no adverse reactions whatsoever. One way to account for this is to assume those batches were placebos. Adding credibility to such an assumption is the fact these German scientists discovered “almost none of the harmless batches, unlike the very-bad and not-so-bad batches, appear to have been subject to any quality-control testing at all.” The country’s regulatory agency, the PEI, “tested and approved for release all the very bad ‘blue’ batches, the overwhelming majority of the not-so-bad ‘green’ batches, but almost none of the harmless ‘yellow’ batches – as if the PEI knew in advance that these batches were unproblematic.” It should be pointed out that pharmaceutical products approved by any regulatory agency in any EU member state can then be used throughout the EU without any additional reviews or approval processes. This could be why the yellow batches appeared to have undergone no quality control testing, but it still wouldn’t account for why those batches aligned so closely with the yellow line of best fit. I also believe using placebos would be in the best interest of the greedy, dishonest pharmaceutical companies producing these experimental and unproven injections. Giving a large number of people fake vaccines would contribute greatly to the general belief they are safe, when there have been indications from the very start of the vaccine rollout they are anything but. Update (6/29/23): A doctor named Geoff Pain has apparently taken exception to the conclusions reached by the Daily Sceptic and publishes a rather scathing rebuttal at his Substack. According to Pain, there are numerous reasons to dispute what he refers to as the “Placebo Fantasy,” and provides readers with a lot of information and some decent analysis to support his view. The problem, however, is nothing he provides explains why the batches of COVID jabs (which Pain is clearly not a fan of) distributed in Denmark can fit so snugly into one of three groups. Coincidentally, the German scientists who analyzed the results of the Danish study and suggested the use of a placebo appeared today on a German podcast called “Punkt.PRERADOVIC” to discuss their findings. The interview is in German but has English subtitles – it’s also very interesting. When considering everything, it looks like the curious case of the mysterious placebo jabs lives on. Update (12/1/23): According to Dr. Peter McCullough, the “hot lot theory” has been confirmed.
July 5 – Doctors Peter McCullough, Paul Alexander, Harvey Risch, William Makis and others publish a preprint study in The Lancet titled, “A Systematic Review of Autopsy Findings in Deaths after COVID-19 Vaccination.” The paper looked at 325 autopsies and found “The mean time from vaccination to death was 14.3 days. Most deaths occurred within a week from last vaccine administration. A total of 240 deaths (73.9%) were independently adjudicated as directly due to or significantly contributed to by COVID-19 vaccination.” The doctors interpreted the findings by writing in part, “The consistency seen among cases in this review with known COVID-19 vaccine adverse events, their mechanisms, and related excess death, coupled with autopsy confirmation and physician-led death adjudication, suggests there is a high likelihood of a causal link between COVID-19 vaccines and death in most cases.” Update (7/6/23): The Lancet takes down the study claiming its “conclusions are not supported by the study methodology” and implying it violated their “screening process.” The more likely scenario is The Lancet did not like the study’s conclusion – ya know, because science. I’ve written about some of these doctors quite a bit throughout this timeline and these are people who have been at the top of their fields for years. From the onset of the pandemic these doctors were thinking outside the box and sticking their necks out to help people through off-label prescribing, while The Lancet on the other hand was busy lying to you every chance they got, covering for scoundrels like Peter Daszak and Anthony Fauci, and printing love letters to Chinese scientists. What a sick joke. The full paper can still be read courtesy of The Daily Sceptic. Update 2 (7/9/23): Dr. Peter McCullough joins Jan Jekielek on American Thought Leaders to discuss the study’s findings and why he believes it should not have been taken down.
July 20 – A study out of Switzerland is published in the European Journal of Heart Failure titled, “Sex-specific differences in myocardial injury incidence after COVID-19 mRNA-1273 Booster Vaccination.” The study looked at 777 hospital employees who were scheduled for a Moderna booster jab and later assessed for vaccine-associated myocardial injury through the measurement of their troponin levels. 22 out of the 777 were diagnosed with myocarditis – which is 2.8% or 1 in 35. The study’s authors concluded “mRNA-1273 vaccine-associated myocardial injury was more common than previously thought, being mild and transient, and more frequent in women versus men.” As of May 10th, over 230,600,00 Americans are considered “fully vaccinated.” 2.8% of 230,600,000 is 6,456,800 – which means there are potentially a lot of people out there who could have heart damage and not even know it. For Dr. John Campbell’s breakdown of the study see this. Hat tip to Alex Berenson.
August 1 – A study is published at PubMed titled, “Cardiovascular Assessment up to One Year After COVID-19 Vaccine-Associated Myocarditis.” The aim of the study was to look at the “long-term cardiovascular outcomes” in forty adolescents up to one year after a “COVID-19 vaccine-associated myocarditis” diagnosis. The study found, “Global systolic ventricular function appears to be preserved. However, impairment of LV and RV myocardial deformation and persistence of LGE in a significant subset of patients with up to 1 year of follow-up was observed. Growing evidence suggests worse prognosis in the presence of altered myocardial deformation and LGE in patients with myocarditis. A short-term study reported abnormal CMR-derived LV longitudinal strain and LGE in 70% to 75% of adolescent patients with COVID-19 vaccine-associated myocarditis followed up for 3 to 8 months. Similar CMR findings were found in young adults studied at 3 to 6 months after the initial diagnosis. The implications of impaired systolic and diastolic myocardial deformation and LGE in our patient subset remain unclear. Nonetheless, given that impaired myocardial deformation and LGE are indicators of subclinical myocardial dysfunction and fibrosis, there exists a potential long-term effect on exercise capacity and cardiac functional reserve during stress.” Could this explain why countless athletes have been collapsing – and in many cases dying – over the past two years? Also see this.
August 8 – A study is published at the Cureus website titled, “COVID-19 Excess Deaths in Peru’s 25 States in 2020: Nationwide Trends, Confounding Factors, and Correlations With the Extent of Ivermectin Treatment by State.” Researchers found “Reductions in excess deaths over a period of 30 days after peak deaths averaged 74% in the 10 states with the most intensive IVM use. As determined across all 25 states, these reductions in excess deaths correlated closely with the extent of IVM use. During four months of IVM use in 2020, before a new president of Peru restricted its use, there was a 14-fold reduction in nationwide excess deaths and then a 13-fold increase in the two months following the restriction of IVM use. Notably, these trends in nationwide excess deaths align with WHO summary data for the same period in Peru.The natural experiment that was put into motion with the authorization of IVM use for COVID-19 in Peru in May 2020, as analyzed using data on excess deaths by locality and by state from Peruvian national health sources, resulted in strong evidence for the drug’s effectiveness. Several potential confounding factors, including effects of a social isolation mandate imposed in May 2020, variations in the genetic makeup of the SARS-CoV-2 virus, and differences in seropositivity rates and population densities across the 25 states, were considered but did not appear to have significantly influenced these outcomes.” Francisco Sagasti was the president who stopped government distribution of ivermectin to Peruvian citizens, which was how most people were getting it. I don’t know too much about him, but I’d bet dollars to donuts his interests are aligned with those of the global death cult.
August 11 – A study is published in eBioMedicine titled, “Differences in SARS-CoV-2 specific humoral and cellular immune responses after contralateral and ipsilateral COVID-19 vaccination.” The study found “Both ipsilateral and contralateral vaccination induce a strong immune response [according to them – not me], but secondary boosting is more pronounced when choosing vaccine administration-routes that allows for drainage by the same lymph nodes used for priming. Higher neutralizing antibody activity and higher levels of spike-specific CD8 T-cells may have implications for protection from infection and severe disease and support general preference for ipsilateral vaccination.” In other words, taking a booster jab in the same arm you received the original COVID vax doses will make the ineffective shots more effective.
August 15 – A study is published at the Wiley Online Library website titled, “Detection of recombinant Spike protein in the blood of individuals vaccinated against SARS-CoV-2: Possible molecular mechanisms.” Its purpose was to determine how long the spike proteins created after vaccination could be detected in the blood in order to “consider the risks or benefits in continuing to administer additional booster doses of the SARS-CoV-2 mRNA vaccine.” The authors wrote in part, “Using mass spectrometry examination of biological samples, we detected the presence of specific fragments of recombinant Spike protein in about 50% of subjects who received mRNA-based vaccines. In some cases, we found the PP-Spike marker in vaccinated individuals more than 30 days after the vaccine, indicating that it is possible to detect vaccine ‘Spike’ protein even some time after vaccination and in any organic tissue (data in preparation). Based on the results obtained, hypotheses can be made for possible molecular mechanisms of persistence of ‘Spike PP.’ In particular, three hypotheses are possible… 1) It is possible that the mRNA may be integrated or re-transcribed in some cells. 2) It is possible that pseudo-uridines at a particular sequence position, as described in the article, induce the formation of a spike protein that is always constitutively active. But it seems very remote as a hypothesis. 3) It is possible that the mRNA-containing nanoparticle will be picked up by bacteria normally present at the basal level in the blood.” Remember when we were told – repeatedly – that the spike proteins created after receiving the mRNA injection would stay at the injection site and only hang around for a few days before being eliminated from the body? That was a lie. It should also be noted that the authors did not say spike protein production stopped after six months – that was just the last time they checked. Also see this.
August 25 – A study out of Melbourne, Australia is published on the Frontiers in Medicine website titled, “BNT162b2 COVID-19 vaccination in children alters cytokine responses to heterologous pathogens and Toll-like receptor agonists.” The study confirms vaccination against COVID-19 causes a decrease in immunity to other viruses, bacteria and fungi – which is also known as VAIDS (vaccine-acquired immune deficiency syndrome). Scientists took blood from 29 children before their first dose of the “vaccine” and again 28 days after the second dose to “investigate in vitro cytokine responses to heterologous stimulants.” As is the case with most studies seeking to measure how the COVID “vaccines” affect other aspects of a person’s health, the scientists downplayed their own findings with a generic-sounding “conclusion” that reads, “BNT162b2 vaccination in children alters cytokine responses to heterologous stimulants, particularly one month after vaccination. This study is the first to report the immunological heterologous effects of COVID-19 vaccination in children.” A closer look at the data, however, shows a significant decrease in natural immune response 28 days after the second dose – many responses to specific pathogens were reduced by a factor of ten. The authors wrote in part, “At V2 + 28, interferon-γ and monocyte chemoattractant protein-1 responses to S. aureus, E. coli, L. monocytogenes, BCG vaccine, H. influenzae, hepatitis B antigen, poly(I:C) and R848 stimulations were decreased compared to pre-vaccination. For most of these heterologous stimulants, IL-6, IL-15 and IL-17 responses were also decreased. There were sustained decreases in cytokine responses to viral, but not bacterial, stimulants six months after BNT162b2 vaccination… Following heterologous bacterial, fungal and viral/TLR agonists stimulation, there was a general decrease in cytokine and chemokine responses in children between V1 and V2 + 28. The largest decreases were seen for IFN-γ and MCP-1. IL-6, IL-15, IL-17 also decreased between V1 and V2 + 28 following stimulation with BCG, H. influenzae, S. aureus, hepatitis B antigen, poly(I:C), and R848. L. monocytogenes stimulation induced IL-15, TNF-α and IP-10 decreases between V1 and V2 + 28. IL-8 responses also decreased between V1 and V2 + 28 following H. influenzae and S. aureus stimulation. RANTES was the only analyte that increased in response to heterologous stimulants (L. monocytogenes and C. albicans) between V1 and V2 + 28… BNT162b2 vaccination is associated with a sustained decrease in cytokine responses to viral, but not bacterial, stimulants six months after vaccination… For viral/TLR agonists (hepatitis B antigen, poly(I:C), R848 stimulations, there were decreases in several cytokine and chemokine responses in children at V2 + 182 compared to V1. Hepatitis B antigen and poly(I:C) stimulation responses were decreased for IL-6, IL-15, TNF-α, GM-CSF, PDGF-BB, VEGF, FGF-basic, IL-10, IFN-γ, IL-2, IL-4, IL-5, IL-9, IL-13, and Eotaxin at V2 + 182 compared to V1. In addition, at V2 + 182 compared to V1, hepatitis B antigen stimulation responses also decreased for IL-1β, IL-12p70, IL-17, and MIP-1β. Poly(I:C) stimulation response to IL-1ra, IL-7, and MIP-1α were also decreased at V2 + 182 compared to V1… Our study showed that, in children, SARS-CoV-2 mRNA vaccination decreases inflammatory cytokine responses (IFN-γ, MCP-1, IL-6, IL-8 and IL-15) to heterologous bacterial, fungal and viral re-stimulation… Our findings suggest SARS-CoV-2 mRNA vaccination could alter the immune response to other pathogens, which cause both vaccine-preventable and non-vaccine-preventable diseases. This is particularly relevant in children as they: have extensive exposure to microbes at daycare, school, and social occasions; are often encountering these microbes for the first time; and receive multiple vaccines as part of routine childhood vaccination schedules… These data show that a SARS-CoV-2 mRNA-based vaccine alters heterologous immunity in children and that these effects can persist up to six months after vaccination… That SARS-CoV-2 mRNA vaccination in children could impact immune responses to other pathogens emphasises the need for further research and consideration of heterologous effects in vaccination policies given their broad public health implications.” Hat tip to Igor Chudov.
August 27 – The UK Daily Mail reports on a study out of South Korea that found N95 masks, which are wrongly believed to be the best defense against viruses, contain toxic chemicals at levels “eight times the recommended safety limit of toxic volatile organic compounds (TVOCs). Inhaling TVOCs has been linked to health issues like headaches and nausea, while prolonged and repeated [exposure] has been linked to organ damage and even cancer.” The researchers who conducted the study said leaving the mask exposed to open air for at least 30 minutes after removing it from its packaging can drastically reduce this exposure – though wearing any mask to protect yourself from COVID is not only unscientific, but harmful (also see this).
September 17 – A study is published by Correlation Research in the Public Interest titled, “COVID-19 vaccine-associated mortality in the Southern Hemisphere.” The study, which is not yet peer-reviewed, looked at data from seventeen “equatorial and Southern-Hemisphere countries” and found “there is no evidence in all-cause mortality (ACM) by time data of any beneficial effect of COVID-19 vaccines. There is no association in time between COVID-19 vaccination and any proportionate reduction in ACM. The opposite occurs. All 17 countries have transitions to regimes of high ACM, which occur when the COVID-19 vaccines are deployed and administered. Nine of the 17 countries have no detectable excess ACM in the period of approximately one year after a pandemic was declared on 11 March 2020 by the World Health Organization (WHO), until the vaccines are rolled out (Australia, Malaysia, New Zealand, Paraguay, Philippines, Singapore, Suriname, Thailand, Uruguay). Unprecedented peaks in ACM occur in the summer (January-February) of 2022 in the Southern Hemisphere, and in equatorial-latitude countries, which are synchronous with or immediately preceded by rapid COVID-19-vaccine booster-dose rollouts (3rd or 4th doses). This phenomenon is present in every case with sufficient mortality data (15 countries). Two of the countries studied have insufficient mortality data in JanuaryFebruary 2022 (Argentina and Suriname)… We quantify the overall all-ages vDFR [vaccine-dose fatality rate] for the 17 countries to be (0.126 ± 0.004) %, which would imply 17.0 ± 0.5 million COVID-19 vaccine deaths worldwide, from 13.50 billion injections up to 2 September 2023. This would correspond to a mass iatrogenic event that killed (0.213 ± 0.006) % of the world population (1 death per 470 living persons, in less than 3 years), and did not measurably prevent any deaths. The overall risk of death induced by injection with the COVID-19 vaccines in actual populations, inferred from excess all-cause mortality and its synchronicity with rollouts, is globally pervasive and much larger than reported in clinical trials, adverse effect monitoring, and cause-of-death statistics from death certificates, by 3 orders of magnitude (1,000-fold greater)… These findings are conclusive. The associations are numerous and systematic, and there are no counter examples. We have found no evidence in our extensive research on ACM that COVID-19 vaccines had any beneficial effect. If vaccines prevented
transmission, infection or serious illness, then there should be decreases in mortality following vaccine rollouts, not increases, as in every observed elderly age group subjected to rapid booster rollouts. And, mortality would not increase solely when vaccines are rolled out, where no excess mortality occurs prior to vaccine rollouts, as we have documented here, in 9 countries across 3 continents.” Wow. Just unreal.
September 22 – A study is published at Science Advances titled, “Unexpected vaginal bleeding and COVID-19 vaccination in nonmenstruating women.” It found women who do not menstruate were several times more likely to experience unexpected vaginal bleeding after receiving the COVID jab. The authors wrote in part, “Our findings indicate that the COVID-19 vaccines, or the host response to them, can lead to vaginal bleeding in a wide range of women. Unexpected vaginal bleeding in post-, peri-, and premenopausal women generally have different underlying causes. However, our findings of an increased risk across the reproductive stages raise the possibility that the mechanisms linking COVID-19 vaccination to unexpected vaginal bleeding may be similar across the stages. Although our data are not fit to explore biological mechanisms, the increased risk after vaccination across different stages of reproductive aging (i.e., in post-, peri-, and premenopausal women) and exogenous hormone use may suggest that the mechanism is not through disruptions of the hypothalamic-pituitary-ovarian axis. Increased risk after both Comirnaty and Spikevax suggest a mechanism related to the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) spike protein and not to other vaccine components.” According to Nature, “The team looked at more than 21,000 responses from postmenopausal, perimenopausal and non-menstruating premenopausal women – including some who were on long-term hormonal contraceptives… They found that 252 postmenopausal women, 1,008 perimenopausal women and 924 premenopausal women reported experiencing unexpected vaginal bleeding. Of these, roughly half of each group said that the bleeding came in the four weeks after the first or second vaccine dose, or both. Premenopausal and perimenopausal women were most likely to report unexpected bleeding in the month after the vaccine, with their risk being three to five times as high as before the vaccinations existed. The risk for postmenopausal women increased by two- to threefold.” Nature even had the audacity to insist that while they can’t explain how or why this is happening, the COVID jabs are “safe and effective.” So scientific.
September 25 – According to an article published in Nature, “Molnupiravir, an antiviral medication widely used against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), acts by inducing mutations in the virus genome during replication. Most random mutations are likely to be deleterious to the virus and many will be lethal; thus, molnupiravir-induced elevated mutation rates reduce viral load. However, if some patients treated with molnupiravir do not fully clear the SARS-CoV-2 infections, there could be the potential for onward transmission of molnupiravir-mutated viruses. Here we show that SARS-CoV-2 sequencing databases contain extensive evidence of molnupiravir mutagenesis… we find that a specific class of long phylogenetic branches, distinguished by a high proportion of G-to-A and C-to-T mutations, are found almost exclusively in sequences from 2022, after the introduction of molnupiravir treatment, and in countries and age groups with widespread use of the drug… To establish the mutational profile induced by molnupiravir, we analysed published longitudinal genomic time series that included both untreated patients and patients treated with molnupiravir, and compared them against a typical SARS-CoV-2 mutational spectrum. In agreement with previous findings, we found that molnupiravir treatment led to a substantial increase… in the rate of mutations and that this increase was highly specific to transition mutations, especially to G-to-A and C-to-T mutations… While C-to-T mutations are relatively common overall in SARS-CoV-2 evolution, G-to-A mutations occur much less frequently; therefore, an elevated G-to-A proportion was especially predictive of molnupiravir treatment.” In my opinion, it’s best to avoid taking part in any aspect of the mass experiment known as the COVID pandemic. Also see this.
September 30 – A study out of Belgium is published at ScienceDirect titled, “Efficacy and safety of in-hospital treatment of Covid-19 infection with low-dose hydroxychloroquine [HCQ] and azithromycin in hospitalized patients: A retrospective controlled cohort study.” The study, which compared hundreds of hospitalized patients treated with HCQ and azithromycin to thousands of control patients, found a “statistically significant reduction in crude mortality rate at 28 days… in the HCQ-group compared to standard of care (16.8% vs 25.9%, p=0.001)… Patients who did not receive HCQ had a 57% higher risk of mortality. A survival benefit in the treatment group was consistent across all age groups… Treatment of COVID-19 using a combination of hydroxychloroquine plus azithromycin was safe and was associated with a statistically significant mortality benefit in the treatment of COVID-19 infection in hospitalized patients. Our findings do not support the current negative recommendations regarding this treatment.” While these findings certainly serve to continue solidifying HCQ as a sensible and effective treatment for COVID, the authors seem to miss the big picture: The medical community is not allowed to use HCQ because it is so effective – allowing its use would mean the end of the emergency use authorization responsible for injecting billions of people with the deadly COVID clot shots. Remember when the deranged people at Surgisphere contributed completely fabricated data to two studies demonizing the use of HCQ as a treatment for COVID in the earliest days of the scamdemic? If you don’t, see the June 4, 2020 entry I wrote about the treachery.
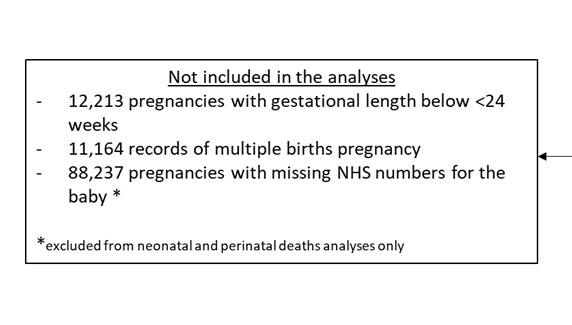
October 9 – A preprint study is published at medRxiv titled, “Covid-19 vaccine safety in pregnancy, a nested case-control study in births from April 2021 to March 2022, England.” Like so many other studies I have written about in this timeline, it does the opposite of what it’s intended to do: prove the COVID clot shots are “safe and effective.” Not only did the study suggest neonatal deaths were 27-32% higher for vaccinated mothers when compared to unvaccinated mothers, but 15% of the vaccinated mothers had a COVID infection during pregnancy versus just 12% in the unvaccinated category. I also suspect the researchers intentionally skewed the results by not including data from over 100,000 pregnancies in their neonatal and perinatal death analysis. By looking at the “data processing flow chart” contained in the supplementary material, you can see over 88,000 pregnancies were excluded because of “missing NHS numbers for the baby,” and more than 12,000 were excluded because the gestational length was less than 24 weeks – which could indicate these women miscarried after taking the jab. Back on June 17, 2021 I linked-to and wrote about a study out of the New England Journal of Medicine which showed “spontaneous abortions” occurred at a rate of 82% when mothers received the COVID vaccine within the first trimester of their pregnancy (which would be less than 24 weeks). It amazes me how many “scientists” seem to be at the beck and call of the death cult.
October 12 – The British Journal of Pharmacology publishes a study which pinpoints how mRNA “vaccines” damage the heart. To conduct their research, scientists from Germany and Hungary “investigated the effect of mRNA-1273 [the Moderna jab] and BNT162b2 [the Pfizer jab] on the function, structure, and viability of isolated adult rat cardiomyocytes [heart muscle cells] over a 72 h period.” The “key results” section of the abstract reads, “In the first 24 h after application, both mRNA-1273 and BNT162b2 caused neither functional disturbances nor morphological abnormalities. After 48 h, expression of the encoded spike protein was detected in ventricular cardiomyocytes for both mRNAs. At this point in time, mRNA-1273 induced arrhythmic as well as completely irregular contractions associated with irregular as well as localized calcium transients, which provide indications of significant dysfunction of the cardiac ryanodine receptor… In contrast, BNT162b2 increased cardiomyocyte contraction via significantly increased protein kinase A… activity at the cellular level.”
The “discussion” section of the study indicates spike protein production in the body may continue longer than we were originally told it would, reading in part, “The rapid and efficient uptake of LNP-mRNA complexes could be reliably demonstrated in both ex vivo perfused Langendorff hearts as well as in human AC16 cardiomyocytes. While our two cell culture systems do not permit any concrete conclusions regarding the duration or extent of spike protein production, all results for AC16 cells indicate a highly efficient and possibly long-lasting translation.”
The authors ultimately concluded “in isolated cardiomyocytes, both mRNA-1273 and BNT162b2 induce specific dysfunctions that correlate pathophysiologically to cardiomyopathy. Both RyR2 impairment and sustained PKA activation may significantly increase the risk of acute cardiac events.”
October 15 – A preprint study is published at medRxiv titled, “Safety of Monovalent BNT162b2 (Pfizer-BioNTech), mRNA-1273 (Moderna), and NVX-CoV2373 (Novavax) COVID-19 Vaccines in US Children Aged 6 months to 17 years.” Using data from “three commercial claims databases,” researchers looked at post-COVID vax “health outcome” data from more than 4M enrollees and found “myocarditis or pericarditis signals were detected following BNT162b2 vaccine in children aged 12-17 years old and seizures/convulsions signals were detected following vaccination with BNT162b2 and mRNA-1273 in children aged 2-4/5 years… Of the two signaled outcomes, the myocarditis or pericarditis signals are consistent with previously published reports. The new signal detected for seizures/convulsions among younger children should be further investigated in a robust epidemiological study with better confounding adjustment.” Children who suffered from post-vax seizures experienced them within a few days of injection, and they happened more frequently in response to the Moderna jabs (which contain more than three times as much mRNA). Despite all of this, the CDC and FDA are still recommending children aged six months and older get injected with up to three doses of this dangerous garbage. Also see this.
October 15 – Another preprint study is published at medRxiv titled, “Evaluation of Stroke Risk Following COVID-19 mRNA Bivalent Vaccines Among U.S. Adults Aged ≥65 Years.” It was conducted as a follow-up after a “small official analysis” conducted in January found receiving flu and COVID vaccines at the same time may increase the risk of having a stroke for older individuals. According to XiNN, “It is the second study to find an elevated risk of stroke for seniors after Covid-19 and flu vaccinations given together… the risk identified in the FDA’s study appears to be very small – roughly 3 strokes or transient ischemic attacks for every 100,000 doses given – and the study found it may be primarily driven by the high-dose or adjuvanted flu vaccines, which are specially designed to rev up the immune system so it mounts a stronger response to the shot… Researchers say they are continuing to probe the possible link, but in the meantime, they say everyone should still get vaccinated since any tiny increase in risk of a stroke after vaccination is dwarfed by the increased risk of stroke or other serious outcomes following either a flu or Covid-19 infection.” It might be worth it… if these shots actually worked! Also see this and this.
December 2 – The British Medical Journal publishes a systematic review regarding COVID mask mandates for children. The study concluded, “Real-world effectiveness of child mask mandates against SARS-CoV-2 transmission or infection has not been demonstrated with high-quality evidence. The current body of scientific data does not support masking children for protection against COVID-19.”
December 6 – Scientists from the University of Cambridge (UK) publish research in Nature titled, “N1-methylpseudouridylation of mRNA causes +1 ribosomal frameshifting.” According to the jargon-filled study, more than 1-in-4 people who took the COVID jab subsequently produced junk proteins instead of the spike proteins they were intended to, leading to “off-target cellular immune responses.” While experimenting on mice, scientists found “responses to +1 frameshifted spike peptides were significantly increased in vaccinated mice compared to untreated mice or those vaccinated with ChAdOx nCoV-19, which does not produce antigen from translation of N1-methylpseudouridylated mRNA… These data suggest that +1 frameshifted products encoded in BNT162b2 spike mRNA are T cell antigens for inbred mice, to which off-target immunity can be detected following vaccination.” In other words, the mice were developing immunity to junk proteins because the creation of the desired spike proteins did not occur, though the researchers do not believe this to be harmful or dangerous – a predictable, yet dubious conclusion. For example, when one of the senior authors of the study, Anne Willis, was interviewed by the Telegraph she said their findings “made [mRNA vaccines] a whole lot safer moving forward” and that fixing this issue “massively de-risks this platform going forward.” So then isn’t she saying what has transpired over the last three years was not only unsafe, but risky, too? That doesn’t sound “safe and effective” to me. Also see this and this.
December 12 – A preprint study is published at Figshare titled, “Critical appraisal of multidrug therapy in the ambulatory management of patients with COVID-19 and hypoxemia.” The paper analyzed the results of several peer-reviewed clinical studies showing 119 COVID patients (from the US, Zimbabwe and Nigeria) who had been experiencing hypoxemia (abnormally low concentration of oxygen in the blood) were successfully treated with a combination of drugs while – most importantly – staying out of the hospital and off a ventilator. The patients were given a combination of several drugs including vitamins C and D, ivermectin, doxycycline, nanosilver and zinc. According to Dr. Peter McCullough, who participated in the study, using “the pulse oximeter was a big mistake in the pandemic. We should have relied on clinical assessment, the work of breathing, and mentation… a large fraction of even the most severe cases could have been treated at home with supplemental oxygen and support. The hospitals became a death trap [also see this and this] for COVID-19 victims as families can attest to today.” Asthma treatments like budesonide work great, too.
December 13 – A study out of Sweden shows people with hypochondriasis “have an increased risk of death from both natural and unnatural causes, particularly suicide, compared with individuals from the general population without hypochondriasis.” In more ways than one, “following the science” could become a death sentence if you’re not careful. This Associated Presstitutes article provides a decent summary of the study’s findings.
December 14 – Moderna publishes the results of a study they conducted on the efficacy of their new mRNA-based RSV “vaccine” in “high-risk” patients and they are underwhelming at best. According to the data, “efficacy was 83.7%… against RSV-associated lower respiratory tract disease with at least two signs or symptoms and 82.4%… against the disease with at least three signs or symptoms. Vaccine efficacy was 68.4%… against RSV-associated acute respiratory disease… Participants in the mRNA-1345 group had a higher incidence than those in the placebo group of solicited local adverse reactions (58.7% vs. 16.2%) and of systemic adverse reactions (47.7% vs. 32.9%); most reactions were mild to moderate in severity and were transient. Serious adverse events occurred in 2.8% of the participants in each trial group.” Considering there were only 20 participants out of more than 35K who reported having three symptoms (which equates to an absolute risk reduction of less than 1%) – and the fact RSV is usually indistinguishable from the common cold – it’s probably best to steer clear of Moderna’s new mRNA product. Also see this breakdown by Igor Chudov.
December 17 – Igor Chudov publishes an interesting article about a retracted 2018 study out of New Zealand. Not only did the top researcher fail to disclose an obvious conflict of interest, they inverted their own findings. Once corrected, the data showed HPV vaccination among pregnant women was significantly increasing the risk of premature birth.
December 27 – A study is published in the European Review for Medical and Pharmacological Sciences titled, “Presence of viral spike protein and vaccinal spike protein in the blood serum of patients with long-COVID syndrome.” The conclusion reads, “This study, in agreement with other published investigations, demonstrates that both natural and vaccine spike protein may still be present in long-COVID patients, thus supporting the existence of a possible mechanism that causes the persistence of spike protein in the human body for much longer than predicted by early studies. According to these results, all patients with long-COVID syndrome should be analyzed for the presence of vaccinal and viral spike protein.” The scientists who conducted the study “identified the presence of the viral spike protein in one patient after infection clearance and negativity of COVID-19 test and the vaccine spike protein in two patients two months after the vaccination.”